
History
Female, 48 years old.
Cough and dizziness for 2 months. A right Pcom aneurysm found incidentally by brain MRA in local hospital.
Medical history: HTN for 3 years, on Amlodipine Besylate, well controlled.
Video 1. Severe stenosis on the right pericallosal artery and occlusion of the callosomarginal artery. Wide-necked posterior communicating artery aneurysm with an elongated daughter sac.
Video 2. 3D reconstruction. 三维重建
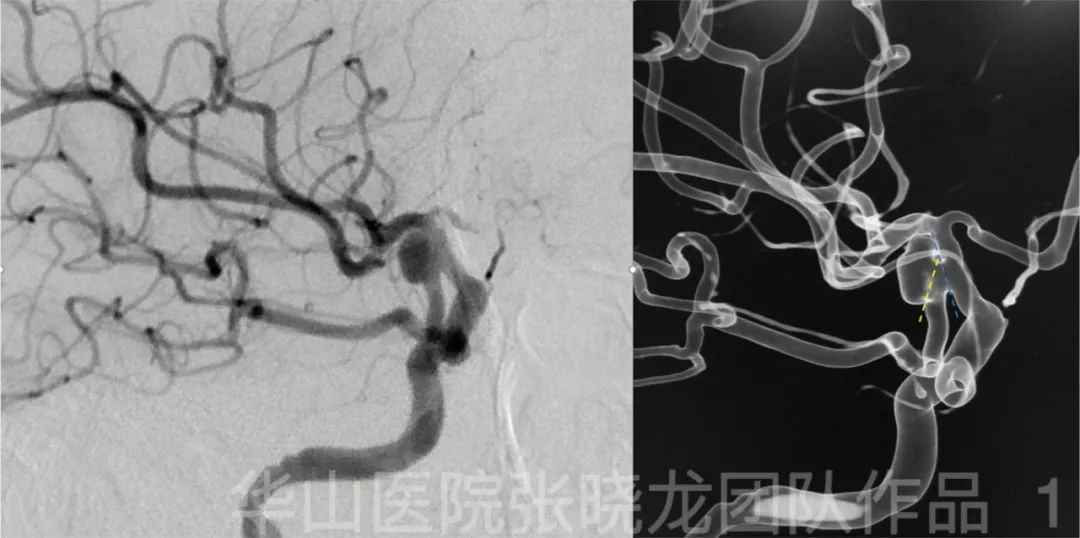
Figure 1. The aneurysm protruded laterally as the Pcom artery heading medially. Therefore two microcatheters were shaped with opposite spiral curve.
01
Operation
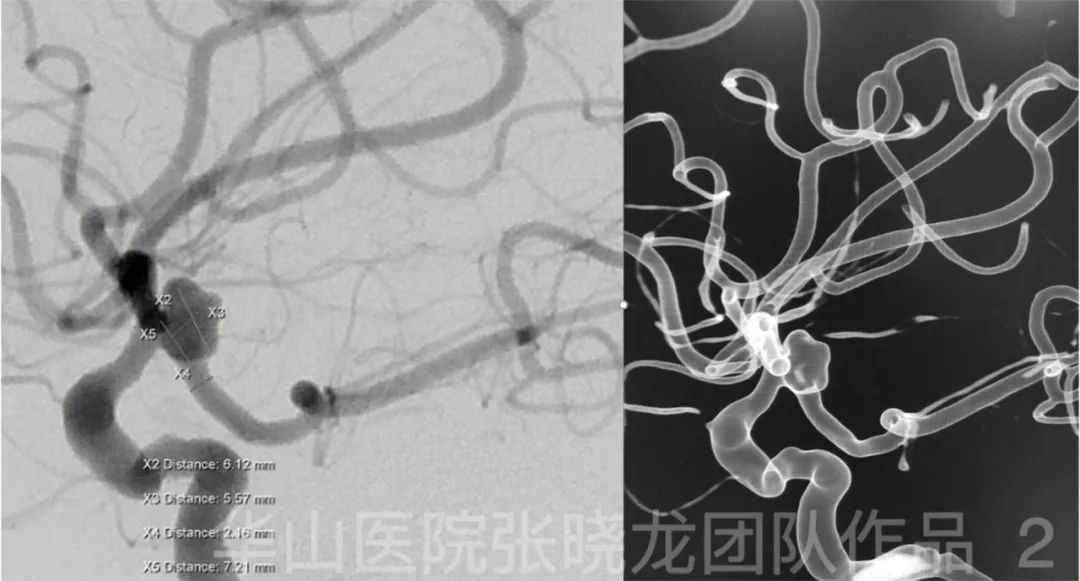
Figure 2. Measurement.
Video 3. After slightly withdrawing the microcatheter, the Transend 205 microwire was advanced into the Pcom artery. Then the microwire tip was re-shaped into an acute curve and was advanced further to PCA. The stenting microcatheter was advanced to distal curve to deploy the stent stably.
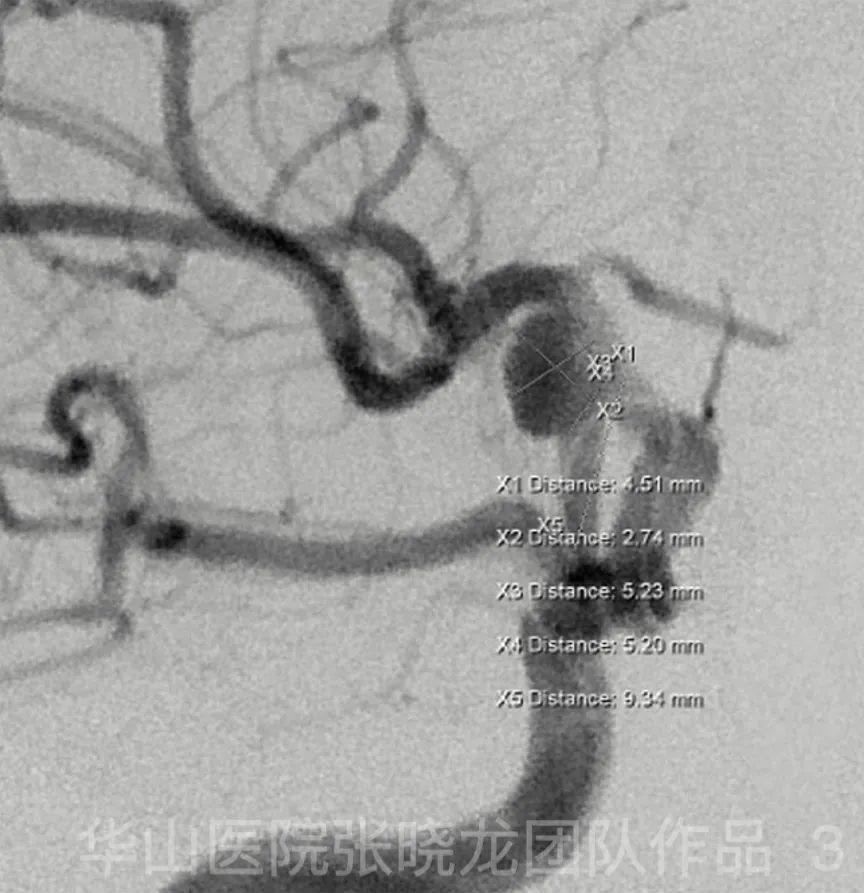
Figure 3. Measurement on the working projection of embolization.

Figure 4 GIF. Echelon-10 for coiling was navigated to the aneurysm sac with the guide of 0.014 microwire. The aneurysmal neck was blocked by the first microcatheter.
Figure 5 GIF. Solitaire 4mm*20mm was placed in the parent artery. The microcatheter for stenting was not retrieved.
Figure 6 GIF. MicroPlex-10 7mm*30cm was inserted for framing.

Figure 7 GIF. Electric detachment of Solitaire was failed. The stent was detached mechanically. General heparinization.
Figure 8 GIF. Angiography shows parent artery patent.

Figure 9 GIF. MicroPlex-10 5mm*15cm was inserted. But a longer coil may pack the dome better.
Figure 10 GIF. Angiography after inserting a MicroPlex-10 4mm*10cm coil shows partially protrusion of coil loops.
Figure 11 GIF. Angiography also indicates loose packing of superior part of the aneurysm.

Figure 12 GIF. HyperSoft 1mm*4cm could not be inserted to the superior loose part of the aneurysm. The aneurysm neck was overpacked instead.
Figure 13 GIF. Rotation angiography shows overpacked aneurysm neck with loose packing of superior part of the aneurysm. The parent artery is patent. Tirofiban 13ml was administrated.
02
Post operative complication
One hour after operation, the patient suffered from slurred speech, left limb muscle strength level I.
Figure 14 GIF. Emergency angiography shows intracranial vessels intact and parent artery patent. Thrombolysis of in-stent thrombosis was considered. Emergency Medication: General heparinization. Tirofiban 12ml iv. Tirofiban 20ml arterially during angiography. Nimodipine 2ml.
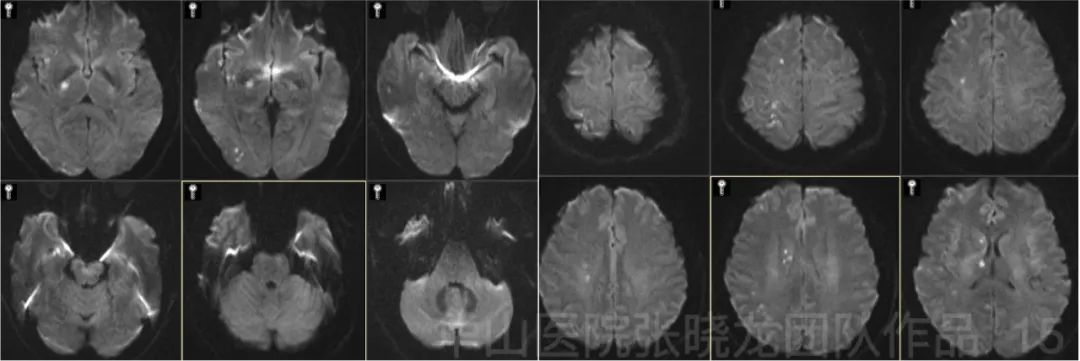
Figure 15. Upper limb muscle strength improved to III. Lower limb V-. MRI DWI shows scattered acute infarctions in the right hemisphere.
03
Post operation
PE: GCS 15, left upper limb III-, left lower limb V-.
Medication: Aspirin 100mg qd, Clopidogrel 75mg qd for 3 months, Amlodipine 5mg qd.
04
Summary
Aneurysm size: 4.51mm*5.23mm; Neck: 2.94mm
Stent: Solitaire 4mm*20mm
Coils: Microplex-10 7mm*30cm, 5mm*15cm, 4mm*10cm (2), Hypersoft 1mm*4cm
For a primitive Pcom artery aneurysm, the neck should not be overpacked. Small thrombus formed in the initial Pcom artery could be flushed into MCA and ACA territory. The thromboembolic events could lead to a disaster.
After the operation, the patient suffered from left weakness, indicating thrombosis in the stent. General heparinization was performed.
05
Follow up records
Long term follow up (2 year): sudden onset of left limbs weakness and dizziness (without numbness) 2 weeks ago. PE: left limbs muscle strength V. Medication: Amlodipine 5mg qd, Zopiclone1/2-1/3# qn.
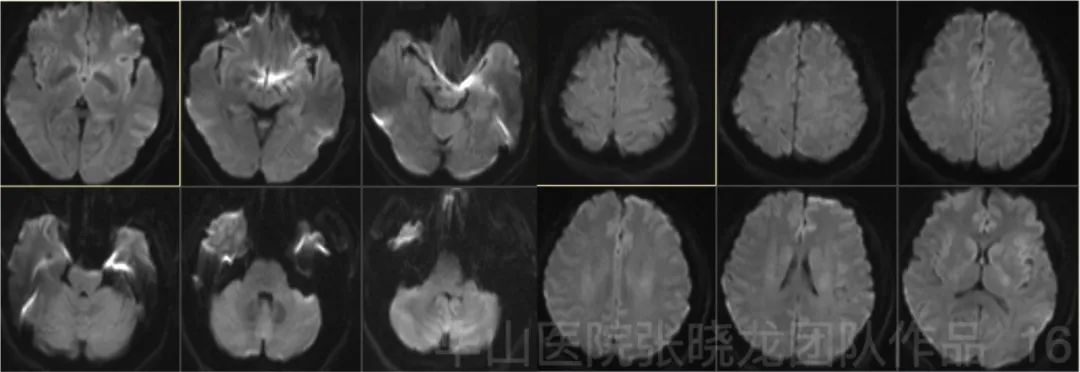
Figure 16. Follow up MRI DWI (3 months) shows no acute infarctions.
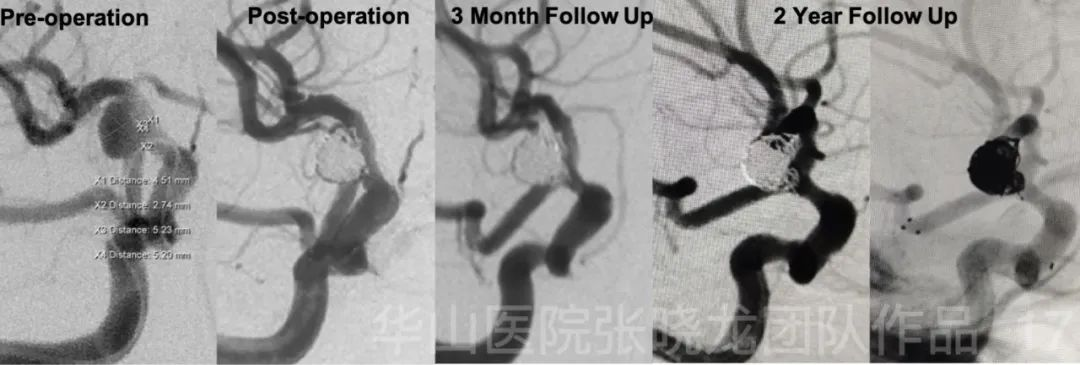
Figure 17. No relapse of the aneurysm during follow up.
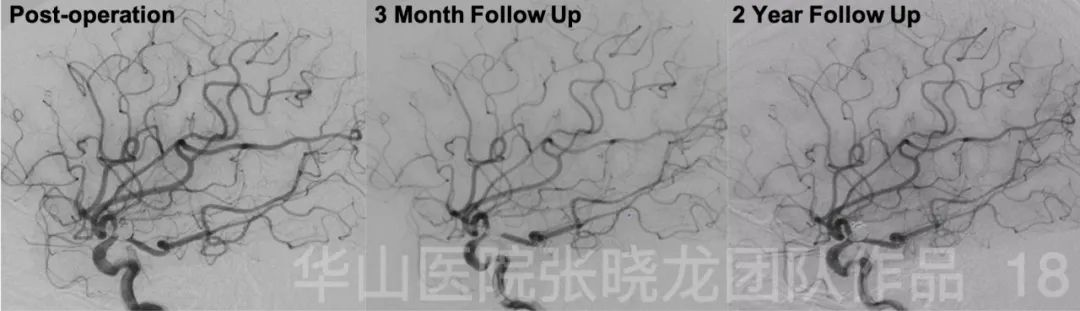
Figure 18. Follow up angiographies show the patent of the parent artery and the intact of intracranial vessels.
06
Summary