
Our case
History
· 74 year-old male
· 2020-10 Suffered from repeated dizziness for four months and local hospital DSA found the right ICA small aneurysm and PICA aneurysm. Then operation was performed in our hospital with aspirin and clopidogrel spanscribed.
· 2021-04 Suffered from mild dizziness.
· PE: left traumatic paralysis, eyelid spasm over 30 years.
· Medical History: Hypertension for 10 years; Diabetes for 10 years; Esophageal cancer, underwent resection and radiotherapy in 2017.
· Medicine: Metoprolol 12.5mg bid, Valsartan amlodipine 1# qd, DMBG 0.5g qd, Acarbose 50mg qd, Glimepiride 4mg qd.
1
Pre-operative
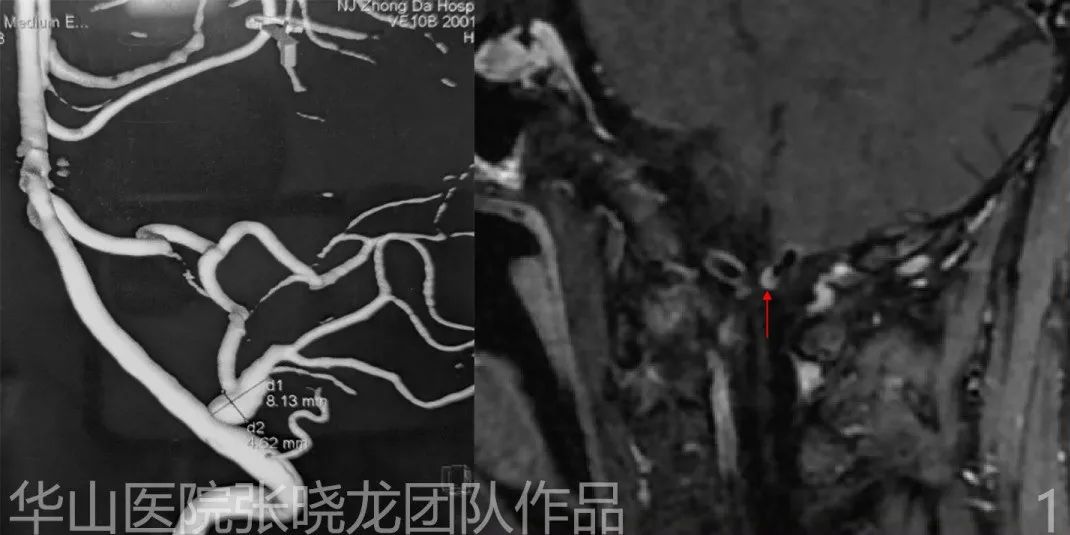
Figure 1. Angiography shows a PICA fusiform aneurysm. HR MRI shows thickening and enhancement of the aneurysm wall.
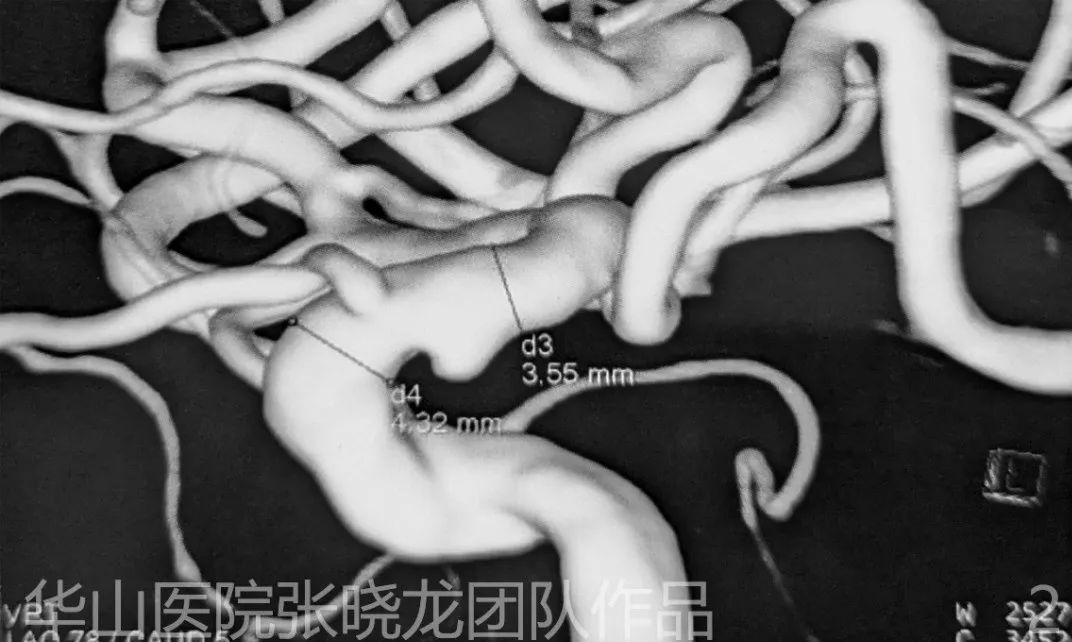
Figure 2. Angiography shows a small ophthalmic aneurysm.
2
Treatment Strategy
· The dominant PICA could be spanserved with large coil frame technique, then the protruded sac would be packed with small coils. Or a solitaire stent could be implanted if the Headway-21 could be advanced across the dissecting aneurysm.
· The small ophthalmic aneurysm could be monitored by follow-up.
3
Operation
Video 1. During angiography of vertebral artery, vasospasm and the small dissection on V3 indicates fragility of the vessel wall. Thus, general heparinization and Nimodipine 1ml were administrated via the guiding catheter. A 6F 70cm long sheath was advanced to the origin of the right vertebral artery.

Figure 3. A DAC 057 catheter was advanced to the origin of the PICA with the guide of a Gateway 2*9mm balloon.

Figure 4 GIF. Headway 21 microcatheter was navigated to the PICA with Synchro-2 Soft microwire.
Video 3. Re-performed the microcatheter roadmap. The tip of the microwire was very difficult to shift upward, therefore we changed into a Synchro-2 standard microwire. The tip of the microwire was shaped into a S curve. After the microwire was shifted upward, directly pushed the wire and waited until the tension was released, then the microwire could be advanced distally.

Figure 5 GIF. The Solitaire 4mm*20mm stent was deployed from the distal bifurcation.
Figure 6 GIF. Nimodipine 1ml was administered via guiding catheter after stenting. Re-performed the rotation.
Figure 7 GIF. Advanced the SL-10 microcatheter into the proximal tip of the Solitaire stent, then the tip of the microwire was shaped almost straight in order to advance through the stent lumen.
Figure 8 GIF. Superselective angiography shows the microcatheter tip is in the lumen of vessel wall.
Figure 9A GIF. Repeated adjust the tension with microwire.

Figure 9B GIF. Repeated adjust the tension with microwire.

Figure 10 GIF. Target 3mm*6cm.

Figure 11 GIF. Target 3mm*4cm.
Figure 12 GIF. Target 2.5mm*6cm.

Figure 13 GIF. Target 2mm*8cm.
Figure 14 GIF. Angiography shows flow detention of the parent artery. Tirofiban 10ml via the guiding catheter. Tirofiban 3ml Nimodipine 0.5ml (diluted) administered via the microcatheter.

Figure 15 GIF. Post-operative angiography shows densely packing of the aneurysm with the parent artery patent.
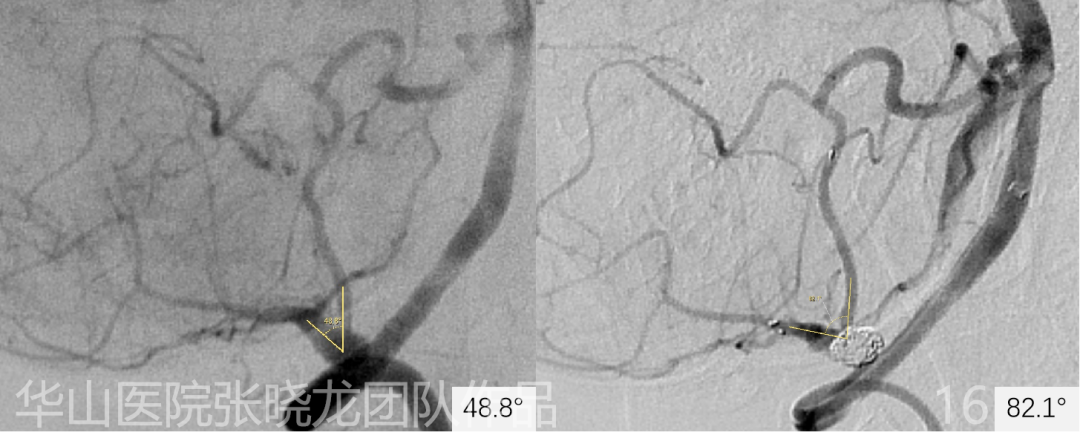
Figure 16. Compared to the span-operative image, the aneurysm angle increases from 48.8 to 82.1 degrees.
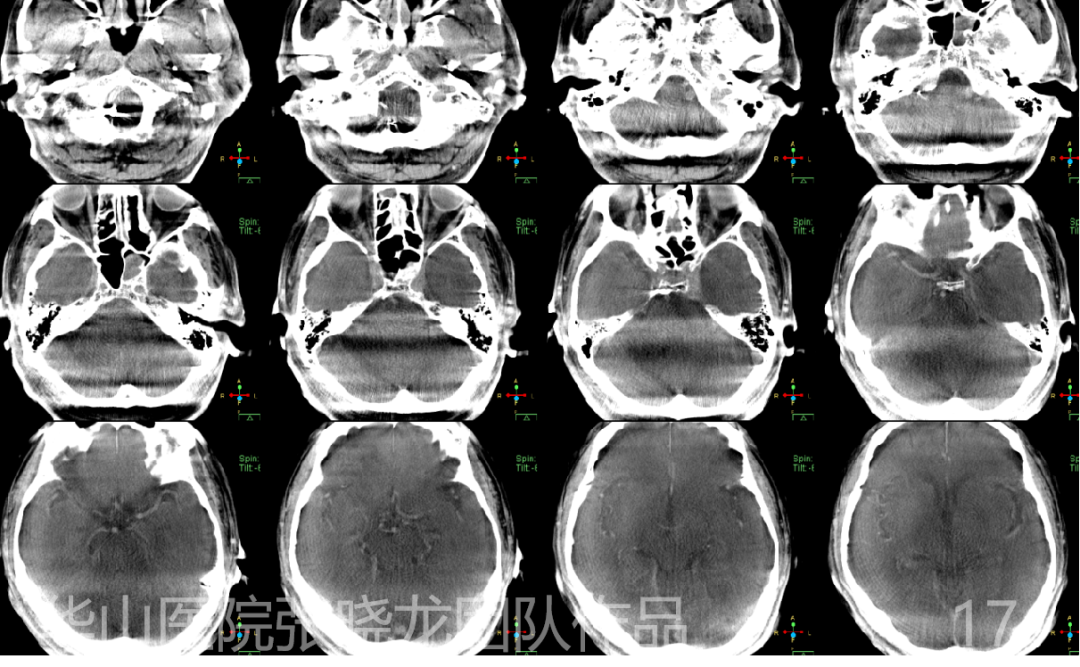
Figure 17. Dyna CT shows no hemorrhage.
4
Post operation
· No neurological deficiency occurred after the procedure.
· PE: GCS 15.
· Medicine: Aspirin 100mg qd, Clopidogrel 75mg qd, Rosuvastatin 10mg qn, Metoprolol 12.5mg bid, Valsartan amlodipine 1# qd, DMBG 0.5g qd, Acarbose 50mg qd, Glimepiride 4mg qd.

Figure 18. Six-month angiography shows no relapse of the aneurysm and the aneurysm angle increases to 85.1°.
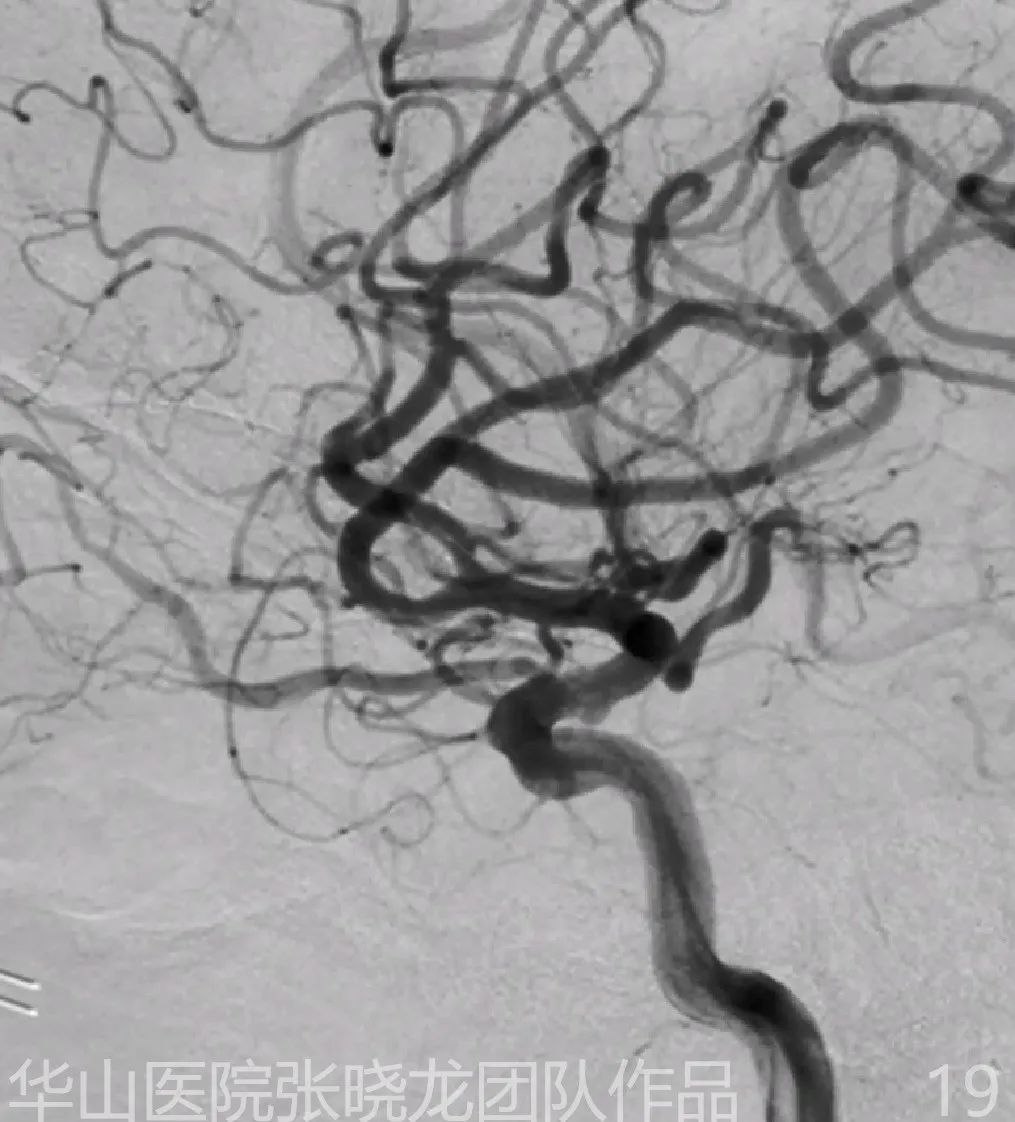
Figure 19. Six-month follow up angiography shows the right ophthalmic aneurysm keeps stable.
5
Follow up
6
Summary
· For a dominant PICA distal dissecting aneurysm, Solitaire stent assisted coiling technique is feasible.
· For a distal dissecting aneurysm with an extremely tortuous parent artery, a steady access route is important.
· A proper length long sheath with a soft guiding catheter can avoid intragenic dissection or thrombosis.
· For a cerebellar parent artery, vascular displacement occurred significantly during the microcatheter advancement. Therefore, the working projection of each curve should be spanpared before the procedure.
· The roadmap via microcatheter should be reperformed while proximal vascular displacement occurred.
· After the microcatheter has passed through several curves, the tension would added in the proximal portion, therefore the tension of the microcatheter should be decreased and added repeatedly to keep stability.
· Straightened the proximal segment of the microcatheter can increase the maneuverability of the microwire.
· Solitaire can straighten the parent artery and therefore reduce the recurrence rate.
· To avoid catheter related thrombosis via a distal access route,single catheter technique should be used instead of the jailing technique.The stent could be detached first, then advance the coiling microcatheter through the stent mesh.