
1.51 y/o male, suffered from sudden onset of unconsciousness and seizure on May 26 2021.
2.PE: NIHSS 3, GCS 15; normal muscle strength; normal pupil diameter and light reflex; normal speech; memory deficiency (cognitive assessment: MoCA 21/30 MMSE 21/30).
3.Med history: hypertension; diabetes.
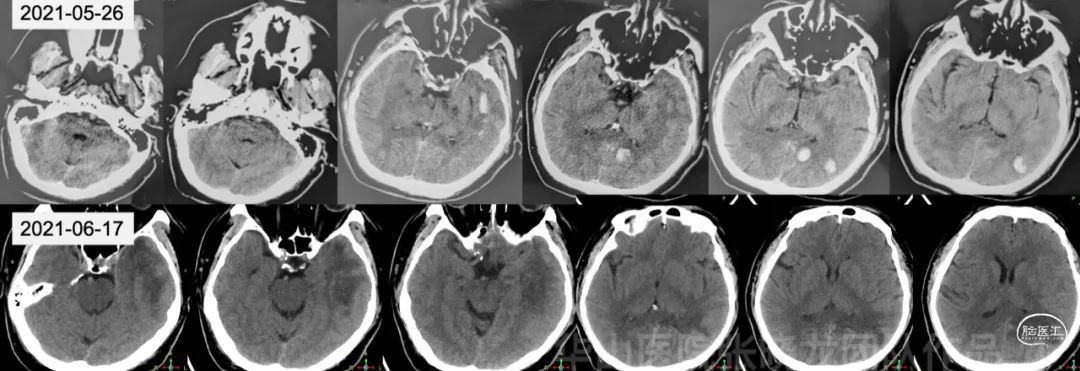
Figure 1
Left temporal and occipital lobe hemorrhage was absorbed at the time of admission to our department.
Figure 2 GIF
Dynamic CE MR demonstrated a fistulous isolated left sigmoid sinus. The Cognard scale was 2a+2b (aggressive). T2 HyperCube images showed multiple hematoma and edema.
Figure 3 GIF
SWI SWAN revealed cerebral and cerebellar venous ectasia.

Figure 4 GIF
TOF MRA demonstrated the left transverse and sigmoid sinus occlusion.
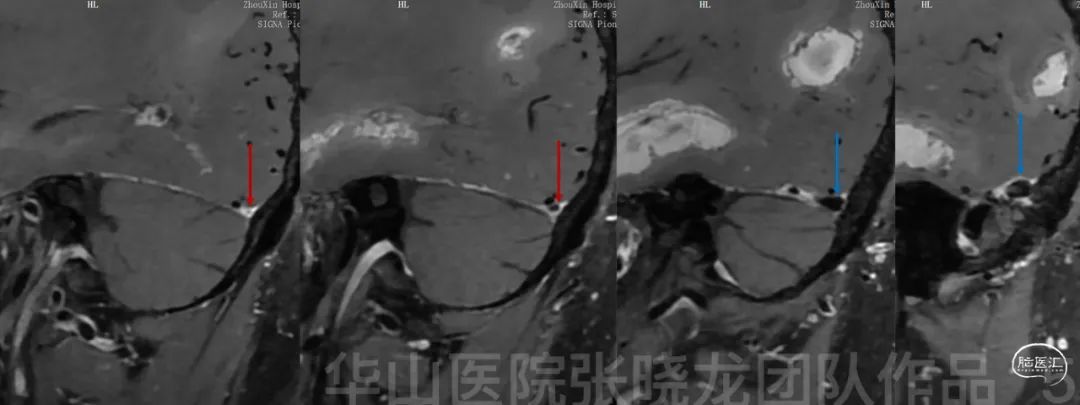
Figure 5
Underdeveloped left TS on sagittal reconstructed images (red arrow). Left residual sigmoid sinus (blue arrow).
Video 1
Left isolated sigmoid sinus fistula was fed by the left ECA refluxed to the cortical veins.
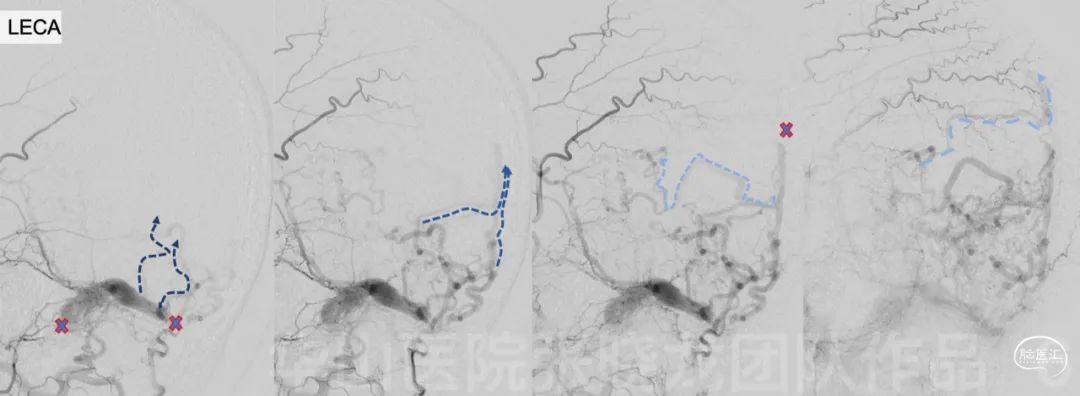
Figure 6
The occipital cortical veins can only reflux into the deep pial venous system due to the occlusion (thrombosis) of the bridging veins on the convex.

Figure 7
After correlation with CE-MR, the left proximal sigmoid sinus was occluded by the fresh thrombus.

Figure 8 GIF
Left tentorial cerebellar veins drained to the lateral sinus were obstructed, compensating by medial vermian veins.

Figure 9 GIF
Left cavernous sinus thrombosis and left ophthalmic venous reflux
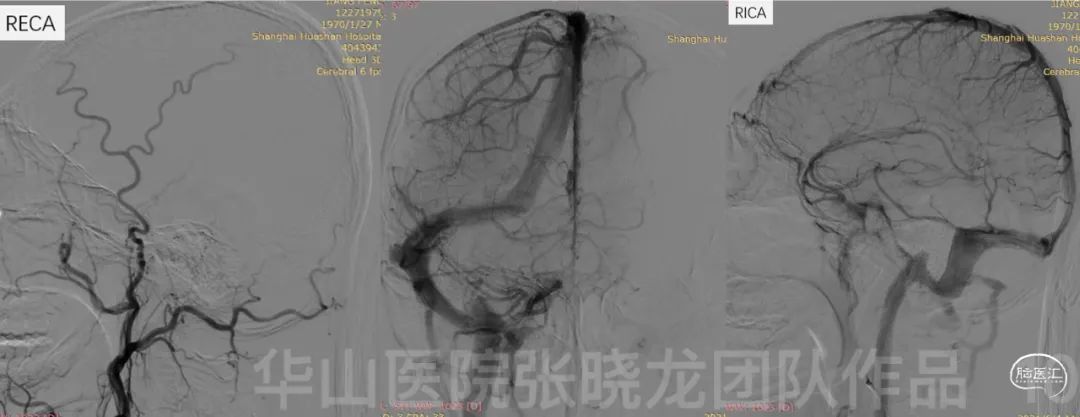
Figure 10
Normal right ICA/ECA, right TS/SS and SSS.
1.Since the fistula was located in the isolated residual left sigmoid sinus with venous reflux, the residual left sigmoid sinus could be recanalized first.
2.The recanalization could be performed retrogradely from the left IJV route;
3. The necessity of the left transverse sinus recanalization should be assessed during the procedure:
-whether the occipital bridging vein would be emptied into the transverse sinus?
-whether the cortical drainage can maintain the patent of the sigmoid sinus?
-direct venography can provide more information on whether the transverse sinus was developed or not.

Figure 11 GIF
The venous guiding catheter was advanced into the residual left sigmoid sinus thrombus, venography demonstrated local occlusion.
Video 2
Fusion images of dual volume reconstruction of the fistulous arteries and veins.

Figure 12 GIF
Distal isolated sigmoid sinus was comparted. A Gateway 4mm*9mm balloon was directly advanced through the thrombus into the distal isolated sinus.
Figure 13 GIF
After dilating the occluded segment by Gateway 4mm*9mm with 8-10 ATM for 3mins, the Envoy DA was advanced over the Gateway to the distal residual sinus. Angiography by the Envoy DA assured that the catheter was in the real lumen of the venous sinus and for the later exchange of a larger balloon or stent.
Video 3
LitePAC 6mm*20mm was exchanged via the Envoy DA and dilated the occlusion with 6 ATM for 2 mins. Partial recanalization of the left sigmoid sinus and the opening of the left Labbe vein are seen.

Figure 14 GIF
Post venous recanalization, left ECA angiography shows the fistula almost vanished.
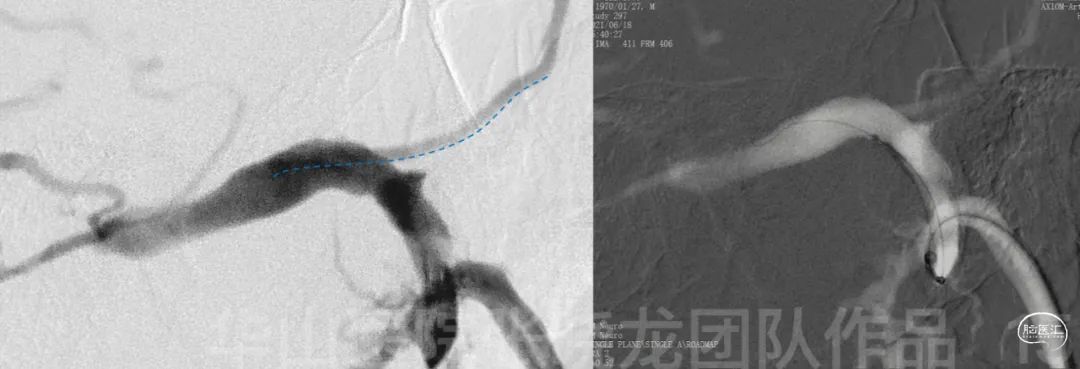
Figure 15
A Precise 7mm*30mm was deployed below the origin of the vein of Labbe. Tirofiban 8ml was given via the venous catheter.

Figure 16 GIF
Postoperative angiography shows nearly complete occlusion of the fistula.
• Postoperative medication: Aspirin and Warfarin for one month. Warfarin for 2 months until follow-up.
• 3 month follow-up.
• INR on 3-mo FU: 2.29, PE on 3mo FU: NS (-)
Figure 17 GIF
Residual fistula in the left sigmoid sinus fed by the left meningohypophyseal trunk, Cognard I.
Figure 18 GIF
Improved venous stasis of left circulation.

Figure 19 GIF
The left transverse-sigmoid sinus has normal drainage function.
Figure 20 GIF
Improved the left cerebellum drainage.
• Warfarin was changed to dual antiplatelet therapy. (Aspirin 100mg qd, Clopidogrel 75mg qd)
• TEG: AA: 97%, ADP: 75%.
Figure 21 GIF
12-month follow up angiography shows complete occlusion of the residual Cognard I fistula.
Figure 22 GIF
Feeder from MHT occluded spontaneously.
Figure 23 GIF
The left sigmoid sinus was patent while no cortical venous stagnation was identified, no cavernous thrombosis and ophthalmic venous reflux.

• This case is a Cognard 2a+2b DAVF with lateral sinus drainage deficiency. The venous connection between the sinus and the vein of Labbe was patent.
• For this thrombus-induced sinus-based-DAVF, a sinus recanalization can release venous hypertension and transfer a high-grade DAVF into a benign low-grade DAVF. Meanwhile, the sinus stenting can compress the dural veins on the sinus wall and block the fistula.
• The lateral sinus DAVF is presented with an isolated sigmoid sinus. The sinus reconstruction includes recanalization of the proximal sigmoid sinus or/and recanalizing the transverse sinus in order to drain the fistula into the contralateral side.
• According to the preoperative contrast enhanced MR, the hyperintensive signal in the left sigmoid sinus indicated acute or subacute occlusion. Meanwhile the MR demonstrated the left transverse sinus is underdeveloped, therefore we preferred proximal sigmoid sinus recanalization. The necessity of TS recanalization should be assessed on whether the cortical vein would drain into the TS. Meanwhile, normal drainage of the left hemisphere can keep the left sigmoid sinus patent.
• A Gateway balloon-guided Envoy DA can simplify the sinus recanalization.
• The fistula almost vanished after the sinus recanalization, which was considered dural venule thrombosis. However, the fistula was recanalized during a 3-month follow-up and the fistula presents as a benign shunt (Cognard 1) due to proximal patency. Therefore, we adjusted the anticoagulation to antiplatelet therapy, and the residual fistula totally occluded within a 12-month follow-up. This case prompted medication adjustment that might be a benefit in residual fistula occlusion and sinus patency.